Inferior pole patellar tendinopathy is almost unheard of in people who are not performing near maximal impact loading. In contrast, you do see quads tendon and distal patellar tendon issues related to compression in people that are no impact loading (e.g. sudden and unaccustomed prolonged kneeling as in DIY activity leading to a compressive quads tendinopathy). That is why this case was interesting. When you are seeing tendinopathies all day, the odd ones are interesting! Here is a brief summary.
56 year old female presented with localized right inferior pole of patella pain (i.e. at the proximal patellar tendon insertion – the typical site of patellar tendinopathy). 3 year history, insidious onset. Worse last few months, ie more consistent pain daily with higher loading activities, eg stairs.
Salient assessment factors
- Single leg decline squat 7/10 pain at 40 degrees – indicative of significant dysfunction and pain issue
- +ve London Hospital Test (ie more pain at the inferior pole when the tendon is relaxed in extension versus stretched in knee flexion – indicates patellar tendon involvement)
- Some tenderness on palpation of Hoffa’s fat pad
- Sleeps on back, BUT with right knee in 110 degrees of flexion
- Post menopausal, onset of symptoms coincided with peak of menopausal symptoms
- History of psoriasis
- She has a sitting job and is relatively inactive, ie even minimal walking, and has been for some years. Activity level has not changed since her symptoms.
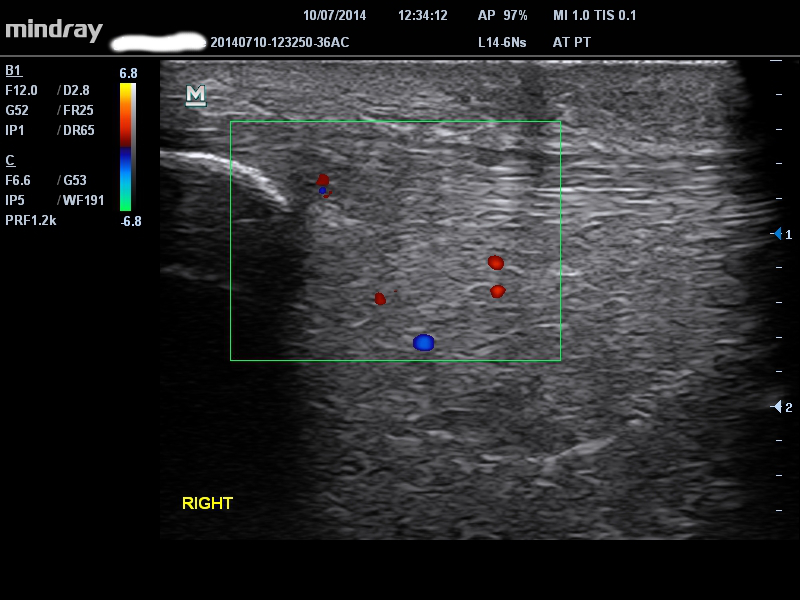
Ultrasound = typical proximal patellar tendon thickening albeit mild
Learning points
1) A reminder that tendinopathy is multi-factorial – It seems for this patient menopause and potential systemic drivers related to psoriasis combined with her unusual and high loading deep knee flexion sleeping position to cause symptomatic patellar tendinopathy.
2) Source of pain can be difficult to differentiate – a significant fat pad component cannot be ruled out, even though her symptoms are localized inferior pole patella. I am mainly suspicious of fat pad because you would expect the quads tendon or distal patellar tendon would be more likely to succumb to compression if deep knee flexion sleep posture is the main load inciting factor.
Management
She has responded very well to:
1) High volume injection to settle irritability
2) Fat pad tape
3) Progressive isometric loading – she had a very good reduction of symptoms immediately following on single leg decline squatting, suggesting that there may be a tendon component
4) Getting her out of knee flexion at night – in my opinion the most important intervention, i.e. changing the one load related factor that she presents with
Conclusion
I’m sure non-load related patellar tendinopathy is seen often in rheumatology clinics. What caught my attention about this case was the interesting load-related factor, ie the sleep position, which always should be assessed carefully in all tendinopathy patients.